
Eight studies. 420 patients. That is the entire pooled evidence base a 2021 meta-analysis could scrape together comparing pulsatile gonadorelin against the older gonadotropin approach in men who needed their testes working again [4]. And after all that pooling, the result was a tie. Not “gonadorelin wins.” A tie, on the outcomes that should matter most: overall success rate, sperm concentration, pregnancy. Faster, yes. Gentler on the estrogen side, yes. But not more likely to get a man to the finish line.
I bring this up first because it is the single most useful number in the whole gonadorelin-versus-HCG argument, and it gets buried under a mountain of confident opinion. If you are on testosterone, or heading there, someone has told you one of these two drugs is obviously the smarter pick. I’d bet money they didn’t mention the tie.
Let me walk you through the actual numbers, because they tell a more interesting story than the hype does, and it is a story with a real “but” in the middle of it.
Why either drug exists at all
Quick mechanics, because the rest of this only makes sense once you have it. Take testosterone from outside your body and your brain reads the abundance and stops sending luteinizing hormone, LH, down to your testes. No LH, no signal, and the testes idle: they shrink, they make less native testosterone, and for a lot of men, they stop producing sperm well. Fine for some guys. Not fine at all for anyone who wants fertility preserved, now or someday, or who just doesn’t want to lose testicular size.
Gonadorelin and HCG both exist to keep that signal alive. They just do it from different addresses in the chain.
One mechanical fact explains almost everything
Here is the chain: hypothalamus sends GnRH, pituitary sends LH, testes respond with testosterone and sperm.
Gonadorelin is a lab-made copy of GnRH. It sits at the very top, nudging your own pituitary to do its job. HCG mimics LH and skips straight to the testes, bypassing the pituitary altogether. One rung of difference in an otherwise identical chain, and nearly every argument you’ll hear about these two drugs traces back to that single rung. Neither is inherently “more natural” in a way that guarantees it works better. They’re two doors into the same room.
What the data supports, and where it quietly stops supporting anything
The strongest published gonadorelin evidence comes from a narrow population: men with congenital hypogonadotropic hypogonadism (CHH), whose own GnRH signal never fired in the first place. Delivered through a programmable pump that mimics the body’s natural rhythm, it performs well in that group. A 2025 study followed 54 such men and watched mean testosterone climb from a hypogonadal baseline around 48 ng/dL to roughly 361 ng/dL at one year, with sperm turning up in about 79 percent of those tested [1]. A 2024 study took 28 men who had already failed standard combined gonadotropin therapy, switched them to pulsatile GnRH, and got about 61 percent producing sperm [2]. That’s a legitimate track record, better than most peptides can claim.
But notice who these men are. They are not the typical guy on TRT giving himself a small maintenance shot. They’re CHH patients on a pump. The mechanism transfers. The trial results don’t, not cleanly.
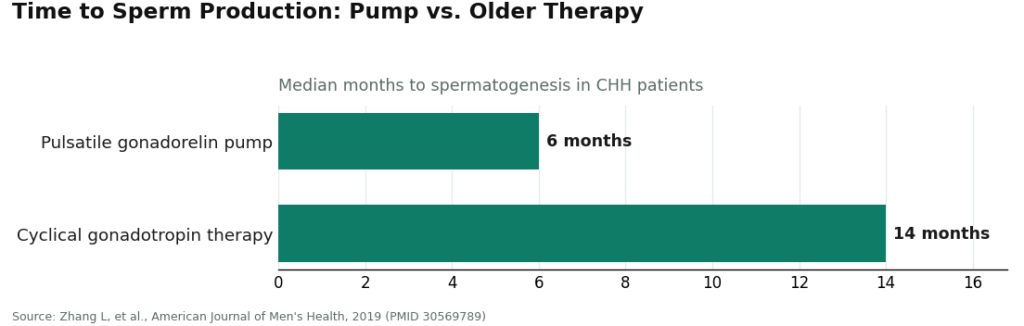
Which brings me back to the head-to-head number I opened with. A 2019 study comparing pulsatile gonadorelin against the older cyclical gonadotropin therapy found gonadorelin got men to sperm production faster, a median of about 6 months against 14 [3], but overall success rates landed about the same. Then the 2021 meta-analysis confirmed it at scale: 8 studies, 420 patients, earlier spermatogenesis, fewer estrogen-related side effects, and no statistically significant edge in the rate of actually getting there [4].
Read that twice. Faster is not the same as better. If anyone tells you gonadorelin is “proven superior,” they are quoting a claim the data doesn’t back. The honest position is duller and truer: both are reasonable, and nobody has run the large trial that would crown a winner in actual TRT patients rather than CHH men on a pump.
See also: The Rise of Encrypted Email
The counterpoint: speed is not nothing
Here’s where I push back on my own tidy “it’s a tie” framing, because a tie on success rate is not a tie on everything. If you’re a man weighing months of your life against months of your life, 6 versus 14 is not trivial. Fewer estrogen-related side effects is not trivial either. A tie in the win column doesn’t erase a real difference in how long the road is or how rough it feels along the way.
So the fair read isn’t “these are identical, take either.” It’s “these trade one advantage for a different kind of certainty,” and that’s a values call, not a science call. Some men will rationally pick speed. Some will rationally pick the deeper track record. Both are defensible readings of the same numbers.
How I’d think about the actual choice
If keeping your whole hormonal axis “exercised” from the top matters to you, gonadorelin’s logic appeals: it asks your own pituitary to do the work rather than substituting for it. Just know about the pulse problem below before you commit to that logic.
If you want the simpler, more predictable poke straight to the testes, HCG has the deeper real-world history on TRT specifically. A lot of the gonadorelin surge over the past few years, frankly, traces back to HCG shortages rather than any proof of clinical superiority. That’s a legitimate reason to reach for gonadorelin. It is a completely different reason from “it works better,” and it’s worth being honest with yourself about which one is actually driving your decision.
If fertility is the actual goal, the tie in the meta-analysis [4] argues for one thing above all: get your labs monitored by a clinician who can watch your real response, rather than betting on a theoretical edge that the biggest available dataset couldn’t confirm.
The detail that gets left out of the pitch
GnRH only works as pulses. Deliver it that way and the pituitary keeps responding. Deliver it as a flat, continuous level, and it does the opposite: it suppresses the pituitary over time. That’s not a fringe worry, it’s the operating principle behind an entire class of drugs designed to shut hormone signaling down deliberately. The studies producing good gonadorelin outcomes used programmable pumps precisely to nail that timing. Most men on TRT are doing scheduled injections, not pump therapy, and getting the rhythm wrong with gonadorelin is a real way to undercut yourself.
HCG doesn’t carry this particular trap, which is a genuine point in its favor on simplicity. It’s not a reason to rule gonadorelin out. It’s a reason to do it under someone’s guidance instead of guessing.
Side effects are real on both sides
Neither drug is a vitamin. Even in monitored gonadorelin research, adverse events showed up: a 2024 safety study of 45 CHH men logged gynecomastia in 8, injection-site hardening in 6, and an allergic reaction in 3 [5]. HCG, by driving up testosterone and therefore estrogen, can produce its own estrogenic side effects, gynecomastia included. None of this is meant to scare you off either option. It’s meant to make sure you go in with someone actually watching your labs. Side effects under supervision are manageable. Side effects nobody is tracking are how people get hurt.
Where to get either one, and why that choice matters as much as the molecule
For gonadorelin specifically, the regulatory picture is worth knowing before you shop around. There is no FDA-approved finished human gonadorelin product on the US market right now. The older branded versions were discontinued for commercial reasons, and the gonadorelin listings still in the FDA’s labeling database today are veterinary [6]. So the legitimate path runs through a compounded preparation, made by a licensed pharmacy, against a real prescription, with a clinician involved in the decision. FormBlends operates on exactly that structure: physician sign-off, licensed-pharmacy compounding, nothing dispensed without a genuine prescription behind it. For a drug where the pick between it and HCG, the dose, and the follow-up labs all depend on a clinician actually reading your numbers, that structure matches the job. To be clear, the compounded product itself is not FDA-approved; what the supervised route buys you is oversight, not a stamp of approval.
The other route, the unprescribed “research use only” vial sold outside the medical system, is cheaper and quicker to get. It’s also a different risk category entirely. No clinician checking your labs, no licensed pharmacy standing behind what’s in the vial, and you alone are responsible for getting the pulse timing right. Plenty of people take that route anyway. If you do, understand the whole burden of verification and timing now sits on you, and for a drug where timing decides the outcome, that’s a heavier burden than the lower price tag suggests.
Where the numbers actually leave us
Gonadorelin and HCG solve the same problem from different points in the chain: gonadorelin at the pituitary, HCG straight at the testes. Gonadorelin has genuine evidence behind it, mostly in CHH men on a pump, and where it’s been tested head-to-head against the older approach, it wins on speed and estrogen tolerability but ties on the outcome that matters most. HCG remains the simpler, longer-established everyday tool, without the pulse-timing trap. Much of the recent gonadorelin enthusiasm has more to do with HCG shortages than with proof of superiority.
Which means the honest answer to “which one is right for me” really is the unglamorous one: it depends on your goal, your labs, and a clinician who is actually watching your response, not a name you pick off a chart because someone sounded certain about it. Choose your sourcing with the same care you’d choose the molecule. Three things stay true no matter which way you lean: the use in men is off-label, the compounded product is not an FDA-approved finished item, and this decision goes better with a clinician who knows your labs in the room for it.
Questions I get asked about this
Is gonadorelin actually better than HCG for fertility on TRT? No one can honestly claim that. There’s no large trial pitting gonadorelin against HCG head-to-head in men on testosterone, so any “clear winner” claim is reaching past what the data shows. The strongest gonadorelin numbers come from CHH patients on a pump, not typical TRT users, and where pulsatile GnRH was tested against older gonadotropin therapy, it got men to sperm production faster but tied on overall success [4]. Both are reasonable choices, and which one fits depends on your goal and your labs.
Why does gonadorelin need to be pulsed while HCG doesn’t? GnRH only keeps the pituitary responsive when it comes in pulses. A flat, steady dose flips that effect and suppresses the pituitary instead, which is the same principle behind certain hormone-shutdown drugs. The trials that produced strong gonadorelin results used programmable pumps to copy that natural rhythm. HCG skips this problem entirely because it acts like LH directly at the testes rather than waiting on the pituitary to respond, which is a real point in its favor for simplicity.
Can I just do scheduled injections instead of a pump? A lot of people on TRT do exactly that, and it’s where things can go wrong without guidance. The strongest gonadorelin results came from pump-delivered pulses, and getting the timing off with manual injections can blunt the response or work against you. Doing this under a clinician who tracks your labs is what keeps you from guessing at dosing and timing entirely on your own.
Why is everyone suddenly talking about switching from HCG to gonadorelin? A lot of that shift traces back to supply problems, not evidence of gonadorelin working better. HCG has gone in and out of shortage repeatedly, and when it got hard to find, men and clinics reached for gonadorelin as the available alternative. That’s a fair reason to consider it. It’s a very different reason from clinical superiority, so it’s worth being clear with yourself about which one is actually behind your decision.
Is there an FDA-approved gonadorelin option I can just buy? Not as a finished human product on the US market today. The old branded versions were discontinued for commercial reasons, and the gonadorelin entries still in the FDA’s labeling database now are veterinary [6]. The legitimate path is a compounded preparation from a licensed pharmacy against a real prescription, with a clinician involved. The supervised route buys you oversight, not an approval claim.
Does gonadorelin have real side effects, or is it gentle? It’s not a vitamin. Even in monitored studies, adverse events turned up: a 2024 safety report on 45 CHH men recorded gynecomastia, injection-site hardening, and an allergic reaction across a handful of participants [5]. HCG can produce its own estrogen-driven side effects for the same reason it raises testosterone. Side effects caught early tend to be manageable. Side effects nobody is watching for are where the real risk hides.
References
- Jiang H, et al. “Therapeutic effects of a pulsatile GnRH pump on adult male patients with congenital hypogonadotropic hypogonadism (CHH): a retrospective study.” Translational Andrology and Urology, 2025. PMID 40800099. https://pubmed.ncbi.nlm.nih.gov/40800099/
- Huang Z, et al. “Pulsatile gonadotropin releasing hormone therapy for spermatogenesis in congenital hypogonadotropic hypogonadism patients who had poor response to combined gonadotropin therapy.” Archives of Endocrinology and Metabolism, 2024. PMID 38739523. https://pubmed.ncbi.nlm.nih.gov/38739523/
- Zhang L, et al. “The Pulsatile Gonadorelin Pump Induces Earlier Spermatogenesis Than Cyclical Gonadotropin Therapy in Congenital Hypogonadotropic Hypogonadism Men.” American Journal of Men’s Health, 2019. PMID 30569789.
- Wei C, et al. “Spermatogenesis of Male Patients with Congenital Hypogonadotropic Hypogonadism Receiving Pulsatile Gonadotropin-Releasing Hormone Therapy Versus Gonadotropin Therapy: A Systematic Review and Meta-Analysis.” The World Journal of Men’s Health, 2021. PMID 32777865.
- Niu YH, et al. “Effect and safety of pulsatile GnRH therapy for male congenital hypogonadotropic hypogonadism.” Zhonghua Nan Ke Xue (National Journal of Andrology), 2024. PMID 39210488.
- U.S. National Library of Medicine, DailyMed. Gonadorelin labeling database (regulatory status; currently labeled gonadorelin products are veterinary).
Written by Ciaran Okafor, health editor. Checking each figure against the cited source. Last reviewed February 2026.
For education, not prescription. Consult a healthcare professional before you begin anything new.